CE Medical Group Blog Post
2021 E/M Updates
By Melissa Billman, Director of Billing at CE Medical Group
There are many billing and coding updates coming in 2021 to be prepared for. SPPM and C E Medical Group has collaborated to help summarize them for you. Here are the key changes highlighted in this post.
Key Changes to E/M Coding:
- 99201 has been deleted.
- History and physical exam as elements for code selection was eliminated.
- More Additional detail added to coding description and guidelines to promote payer consistency.
- Guidance added on when comorbidities and underlying diseases are to be counted for medical decision making.
- Physicians now choose whether they document based on MDM or total time.
AMA states the key reasons behind the changes are:
- “Eliminating history and physical exam as elements for code selection. While significant to both visit time and medical decision-making, these elements alone should not determine a visit’s code level.
- Allowing physicians to choose whether their documentation is based on medical decision-making or total time. This builds on the movement to better recognize the work involved in non-face-to-face services like care coordination.
- Changing medical decision-making criteria to move away from simply adding up tasks to instead focus on tasks that affect the management of a patient’s condition.”
| CURRENT E/M Coding | 2021 Coding Changes |
| History | Total time OR |
| Exam | Medical Decision Making |
| Medical Decision Making |
VERBIAGE CHANGE GUIDELINES
TIME CHANGES
Currently states: Typical face-to-face time
2021 states: Total time spent on the day of the encounter
- 99202: 15-29 minutes of total time is spent on the date of the encounter.
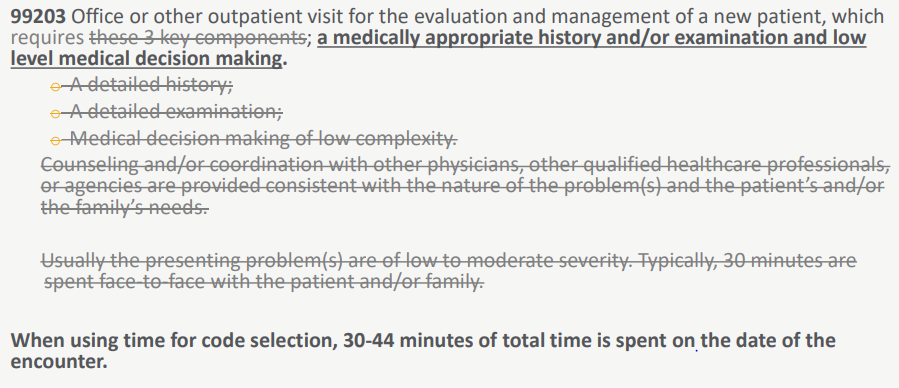
- 99203: 30-44 minutes of total time is spent on the date of the encounter.
- 99204: 45-59 minutes of total time is spent on the date of the encounter.
- 99205: 60-74 minutes of total time is spent on the date of the encounter.
- 99212: 10-19 minutes of total time is spent on the date of the encounter.
- 99213: 20-29 minutes of total time is spent on the date of the encounter.
- 99214: 30-39 minutes of total time is spent on the date of the encounter.
- 99215: 40-54 minutes of total time is spent on the date of the encounter.
What does “total time on date of the encounter” mean?
- Non face-to-face activities are now recognized as “billable” time.
- Exact ranges with specific time increments are given. No longer using the terms “midpoint” or “threshold”.
- Code selection is used when billing based on time (not a required minimum amount when using MDM coding).
- Time spent by clinical ancillary staff is not included in time.
- If more than one clinician addresses the patient, only count 1 clinician per minute.
Physician/Other Qualified Healthcare Professional Time Includes:
- Obtaining and/or reviewing separately obtained history.
- Preparing to see the patient (reviewing tests results, viewing imaging).
- Performing a medically appropriate exam and evaluation.
- Counseling and educating the patient as well as family and/or caregiver.
- Ordering of medications, tests and/or procedures.
- Documenting clinical information in the electronic or other health record.
Not separately reported options:
- Referring and communicating with other health care professionals
- Care coordination.
- Independently interpreting results and communicating results to the patient, family and/or caregiver.
Prolonged Service Code (99417)
Prolonged Services/Prolonged Service with or Without Direct Patient Contact on the Date of an Office or Other Outpatient Service
- Prolonged office or other outpatient evaluation and management service(s) beyond the total minimum required time of the primary procedure which has been selected using total time), requiring total time with or without direct patient contact beyond the usual service, on the date of the primary service, each 15 minutes. List separately, in addition to codes 99205, 99215 for office or other outpatient Evaluation and Management services. Use 99417 in conjunction with 99205, 99215. Do not report 99417 in conjunction with 99354, 99355, 99358, 99359, 99415, 99416. Do not report 99417 for any time unit less than 15 minutes.
Table AMA 2021 CPT Professional CPT
| Duration of Prolonged Service | Report Codes for New Outpatient 99205 (60-74 minutes) |
| Less than 75 minutes | 99205 (99417 not separately reported) |
| 75-89 minutes | 99205, 99417 |
| 90-104 minutes | 99205, 99417 x2 |
| 105 Minutes or more | 99205, 99417 x3 (or appropriate unites for each additional 15 minutes) |
| Duration of Prolonged Service | Report Codes for Established Outpatient 99215 (40-54 minutes) |
| Less than 55 minutes | 99215 (99417 not separately reported) |
| 55-69 minutes | 99215, 99417 |
| 70-84 minutes | 99215, 99417 x2 |
| 85 minutes or more | 99215, 99417 x3 (or appropriate unites for each additional 15 minutes) |
Per the 2021 Proposed Medicare Physician Fee Schedule
• A minimum of 89 minutes must elapse for 99205
• A minimum of 69 minutes must elapse for 99215
MEDICAL DECISION-MAKING CODING UPDATES
Understanding 2021 History and Exam
- Include a medically appropriate history and/or physical examination when performed.
- Extent of the history and/or physical examination is determined by the treating physician or other qualified healthcare professional reporting the service.
- Clinical or care team may collect information and the patient may supply information directly. It must be reviewed by the reporting physician or other qualified healthcare professional. Examples of this would be using a patient portal or a questionnaire.
- The extent of the history and physical examination is not an element in selecting of office or other outpatient services.
| CURRENT GUIDELINES | 2021 E/M GUIDELINES (OFFICES OR OTHER OUTPATIENT) |
| NUMBER OF DIAGNOSIS OR MANAGEMENT OPTIONS | NUMBER AND COMPLEXITY OF PROBLEMS ADDRESSED AT THE ENCOUNTER |
| AMOUNT AND/OR COMPLEXITY OF DATA TO BE REVIEWED | AMOUNT AND/OR COMPLEXITY OF DATA TO BE REVIEWED AND ANALYZED |
| RISK OF COMPLICATIONS AND/OR MORBIDITY OR MORTALITY | RISK OF COMPLICATIONS AND/OR MORBIDITY OR MORTALITY OF PATIENT MANAGEMENT |
Number and Complexity of Problems Addressed at the Encounter
- Symptoms may group around a specific diagnosis, buteach symptom is not necessarily a unique condition.
- Comorbidities/underlying diseases, in and of themselves, are not considered in selecting a level of E/M services unless they are addressed, and their presence increases the amount and/or complexity of data to be reviewed and analyzed or increased risk of complications and/or morbidity or mortality of patient management.
- The final diagnosis for a condition does not in itself determine the complexity or risk. An extensive evaluation may be required to reach the conclusion that the signs or symptoms do not represent a highly morbid condition.
- Multiple problems of a lower severity may, in the aggregate, create higher risk due to interaction.
Problem addressed: A problem is addressed or managed when it is evaluated or treated at the encounter by the physician or other qualified health care professional reporting the service. This includes consideration of further testing or treatment that may not be elected.
Important to know:
- Documenting in the patient’s medical record that another professional is managing the problem without additional assessment or care coordination does not qualify as being ‘addressed’ or managed by the physician or other qualified health care professional reporting the service.
- Referral without evaluation (by history, exam, or diagnostic studies) or consideration of treatment does not qualify as being addressed or managed by the physician or other qualified health care professional reporting the service.
Level 99202 or 99212 (Straightforward)
Must meet 2 of 3 MDM elements
- Number and Complexity of Problems Addressed
- minimal
- 1 self-limited or minor problem
- Amount and/or Complexity of Data to be Reviewed and Analyzed
- Minimal
- None
- Risk of Complications and/or Morbidity or Mortality of Patient Management
- Minimal risk of morbidity from additional diagnostic testing or treatment
2021 Guideline Definitions
- Minimal problem: A problem that may not require the presence of the physician or other qualified healthcare professional, but the service is provided under the supervision of the physician or other qualified health care professional (see 99211).
- Self-limited or minor problem: A problem that runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status.
Level 99203 or 99213 (Low)
Must meet 2 of 3 MDM elements
- Number and Complexity of Problems Addressed
- 2 or more self-limited or minor problems or
- 1 stable chronic illness or
- 1 acute, uncomplicated illness or injury.
- Amount and/or Complexity of Data to be Reviewed and Analyzed (must meet the requirements of at least 1 of the 2 categories)
Category 1: Tests and documents, any combination of 2 from the following:
- Review of prior external notes from each unique source.
- Review of the result of each unique test.
- Ordering of each unique test.
Category 2: Assessments requiring an independent history. For the categories of independent interpretation of tests and discussion of management or test interpretation, see moderate or high).
- Risk of Complications and/or Morbidity or Mortality of Patient Management
- Low risk of morbidity from additional diagnostic testing or treatment
- Risk of Complications and/or Morbidity or Mortality of Patient Management
- Low risk of morbidity from additional diagnostic testing or treatment
- Amount and/or complexity of data to be reviewed and analyzed.
- This data includes medical records, tests, and/or other information that must be obtained, ordered, reviewed, and analyzed for the encounter. This includes information obtained from multiple sources or interprofessional communications that are not separately reported. It includes interpretation of tests that are not separately reported. Ordering a test is included in the category of test results and the review of the test results is part of the encounter and not a subsequent encounter. Data is divided into three categories:
- Tests, documents, orders, or independent histories. (Each unique test, order or document is counted to meet a threshold number.)
- Independent interpretation of tests.
- Discussion of management or test interpretation with external physician or other qualified healthcare professional or appropriate source.
Level 99204 or 99214(Moderate)
Must meet 2 or 3 MDM elements
- Number and Complexity of Problems Addressed
- 1 or more chronic illnesses with exacerbation, progression, or side effects of treatment or
- 2 or more stable chronic illnesses or
- 1 undiagnosed new problem with uncertain prognosis or
- 1 acute illness with systemic symptoms or
- 1 acute complicated injury.
- Amount and/or Complexity of Data to be Reviewed and Analyzed (must meet the requirements of at least 1 of 3 categories)
- Category 1: Tests and documents (any combination of 3 from the following)
- Review of prior external note(s) from each unique source
- Review of the result(s) of each unique test
- Ordering of each unique test
- Assessment requiring an independent historian(s) or
- Category 2: Assessment requiring an independent historian(s)
- Independent interpretation of a test performed by another physician/other qualified health care professional (not separately reported) or
- Category 3: Discussion of management or test interpretation
- Discussion of management or test interpretation with external physician/other qualified health care professional/appropriate source (not separately reported).
- Category 1: Tests and documents (any combination of 3 from the following)
- Risk of Complications and/or Morbidity or Mortality of Patient Management
- Moderate risk of morbidity from additional diagnostic testing or treatment (examples only).
- Prescription drug management.
- Decision regarding minor surgery with identified patient or procedure risk factors.
- Decision regarding elective major surgery without identified patient or procedure risk factors.
- Diagnosis or treatment significantly limited by social determinants of health.
- Moderate risk of morbidity from additional diagnostic testing or treatment (examples only).
Level 99205 or 99215 (High)
Must meet 2 of 3 MDM elements
- Number and Complexity of Problems Addressed
- 1 or more chronic illnesses with severe exacerbation, progression, or side effects of treatment or
- 1 acute or chronic illness or injury that poses a threat to life or bodily function.
- Amount and/or Complexity of Data to be Reviewed and Analyzed (must meet the requirements of at least 2 of the 3 categories)
- Category 1: Tests and documents (any combination of 3 from the following)
- Review of prior external note(s) from each unique source
- Review of the result(s) of each unique test
- Ordering of each unique test
- Assessment requiring an independent historian(s) or
- Category 2: Assessment requiring an independent historian(s)
- Independent interpretation of a test performed by another physician/other qualified health care professional (not separately reported) or
- Category 3: Discussion of management or test interpretation
- Discussion of management or test interpretation with external physician/other qualified healthcare professional (not separately reported).
- Category 1: Tests and documents (any combination of 3 from the following)
- Risk of Complications and/or Morbidity or Mortality of Patient Management
- High risk of morbidity from additional diagnostic testing or treatment (examples only).
- Decision regarding elective major surgery with identified patient or procedure risk factors.
- Decision regarding hospitalization.
- Drug therapy requiring intensive monitoring for toxicity.
- Decision regarding emergency major surgery.
- High risk of morbidity from additional diagnostic testing or treatment (examples only).
For additional information, please visit https://www.ama-assn.org/system/files/2019-06/cpt-revised-mdm-grid.pdf and https://www.ama-assn.org/system/files/2019-06/cpt-office-prolonged-svs-code-chanes.pdf.
About the author: Melissa Billman is the billing director for C E Medical Group, a nation-wide medical billing firm that specializes in working with pain management, sport medicine, family practice, and orthopedic surgery. In addition to managing her large team of medical billers and coders, she speaks nationally at various billing and coding conferences. Melissa resides in Salt Lake City, Utah with her husband and two children.